
By: Dr. Renato Martins
The increasing adoption of orthodontic aligners reflects a significant shift in patient preferences, driven by enhanced awareness of aesthetic dental solutions, advancements in digital orthodontic technologies, and a growing demand for personalized treatment options. Aligners offer a discreet and comfortable alternative to traditional fixed appliances, positioning themselves as an appealing choice for many patients. However, despite their rising popularity, aligners have not consistently achieved the outcomes originally projected in treatment software.1
Specifically, aligners struggle with certain tooth movements, such as root control,2-6 pure vertical movements2,6,7 and complex antagonistic movements like incisor uprighting combined with intrusion or incisor proclination with extrusion. Additionally, while aligners can correct severe rotation or distalize molars,2,5 their efficiency in executing these movements is often lacking. Aligners typically require significantly more time compared to fixed appliances or when used with supplementary mechanics, making them less effective in achieving timely results for these complex adjustments.
Pure extrusion or extrusion with proclination remains particularly challenging for aligners2,8,9 due to their reliance on the elasticity of the plastic and patient compliance, rather than precise load system found in fixed appliances. In addition to vertical challenges, severe rotations pose significant difficulties for aligners.2,5,6,8-10 Although techniques such as round-tripping, overcorrection, and refinements can increase the reliability of rotational corrections, fixed appliances excel due to their ability to exert the continuous forces and the couples necessary for efficient tooth derotation. Using brackets and wires before aligners to correct severe rotations might establish a favorable starting point for subsequent aligner therapy.
Distalization, particularly in achieving anterior-posterior (AP) corrections, highlights these challenges. While aligners can facilitate distalization of maxillary molars by up to 1.5 mm,2,5 the prolonged time required for such movements can pose issues with patient compliance and treatment efficiency. Fixed appliances or supplemental mechanics, like intermaxillary elastics or skeletal anchorage, can achieve equivalent results much faster, offering a more time-efficient solution.
The hybrid treatment approach leverages the strengths of both fixed appliances and aligners. By starting with fixed appliances to address these challenging movements, practitioners can capitalize on their capabilities for specific adjustments. Once foundational corrections are made, transitioning to aligners offers advantages in aesthetics, comfort, oral hygiene, and patient satisfaction. This strategy enhances treatment efficiency, reduces overall treatment time, and delivers high-quality results tailored to individual needs.
In conclusion, the strategic use of fixed appliances during the initial phase of treatment facilitates complex tooth movements that are difficult or less predictable with aligners alone. Once these corrections are achieved, aligners can take over to fine-tune and finish the treatment, offering a comprehensive solution that addresses both clinical needs and patient preferences. This synergy exemplifies the success of hybrid orthodontics in modern practice. This article aims to explore the hybrid treatment approach that combines the strengths of both aligners and fixed appliances to optimize orthodontic outcomes.
Challenges in Extrusion of Anterior Teeth
Extrusion is recognized as the most challenging movement to control with aligners,2,6 with accuracy rates ranging from 29% to 54%.2,8,9 Research indicates that bite closure when using aligners primarily results from changes in incisor positions, accompanied by minimal alterations in molar positioning.11,12 Furthermore, evaluations of the literature reveal that most of these changes stem from retroclination rather than pure extrusion.12 It is also important to note that tipping is likely the most reliably achieved movement with aligners.6,13 Consequently, it can be concluded that achieving pure extrusion—especially when combined with proclination of the incisors, which represents an antagonistic movement—would be even more difficult, if not nearly impossible.
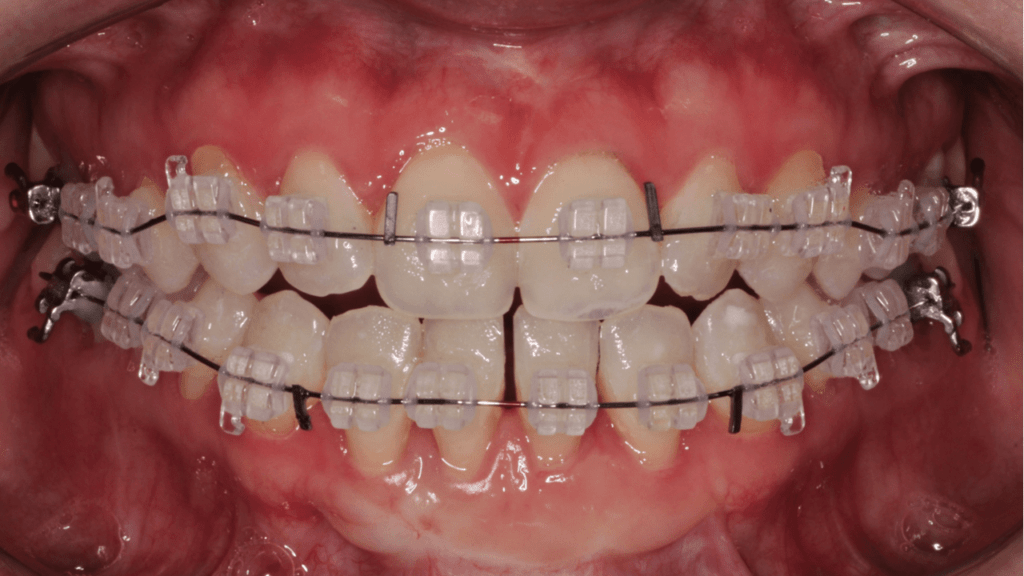
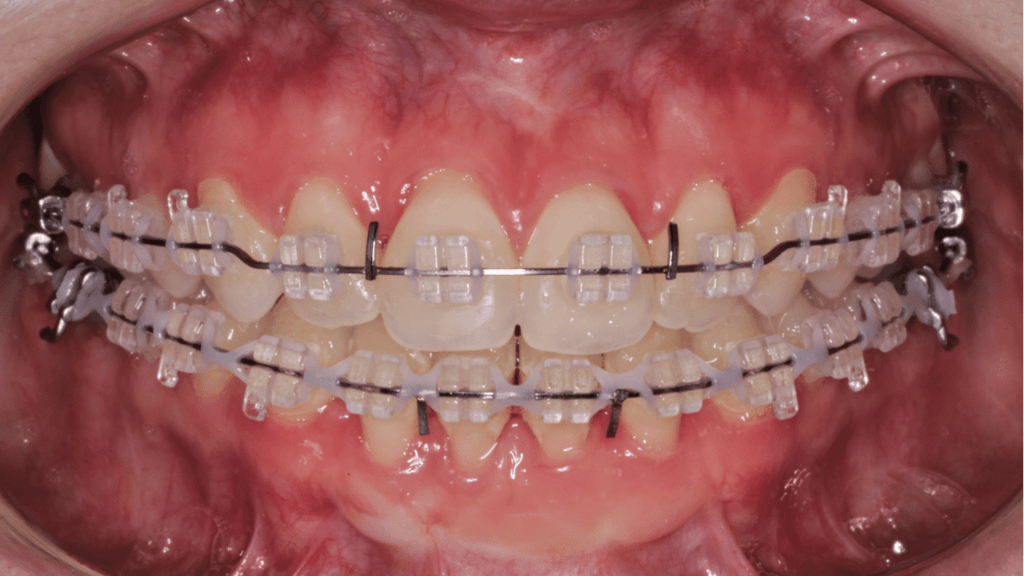
In situations where retroclination of incisors is not permissible or preferred, especially when combined with incisor extrusion, it is advisable to achieve these movements using fixed appliances before commencing aligner therapy. Anterior extrusive mechanics, utilized effectively along with anterior box elastics, 14,15 can facilitate and support the necessary vertical movement in a timely manner. Once the bite has closed effectively, aligners can then be employed to address the remaining aspects of the malocclusion. (FIGURE 1)
Figure 1 – Orthodontic Treatment for Open Bite using hybrid orthodontics


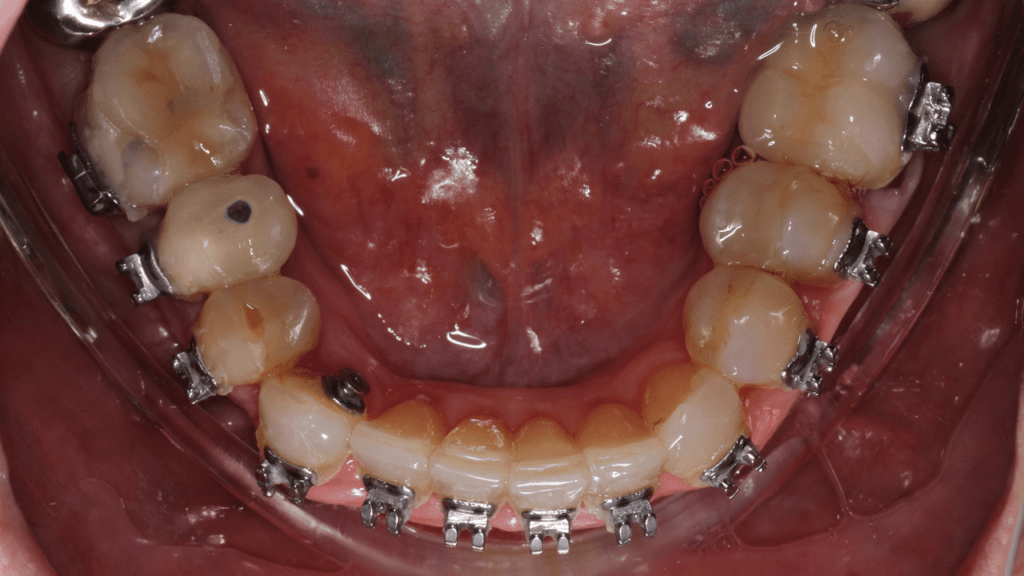
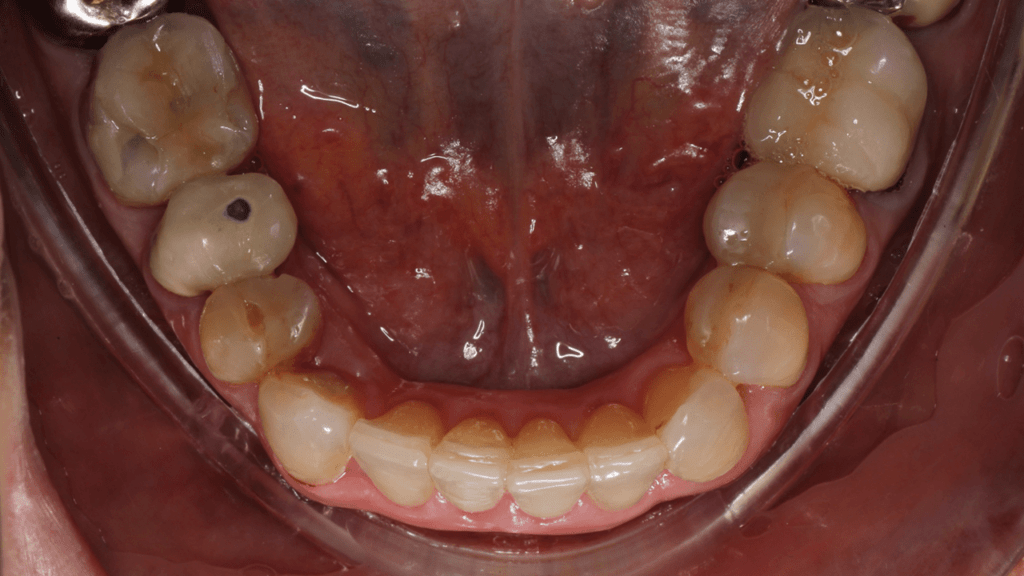
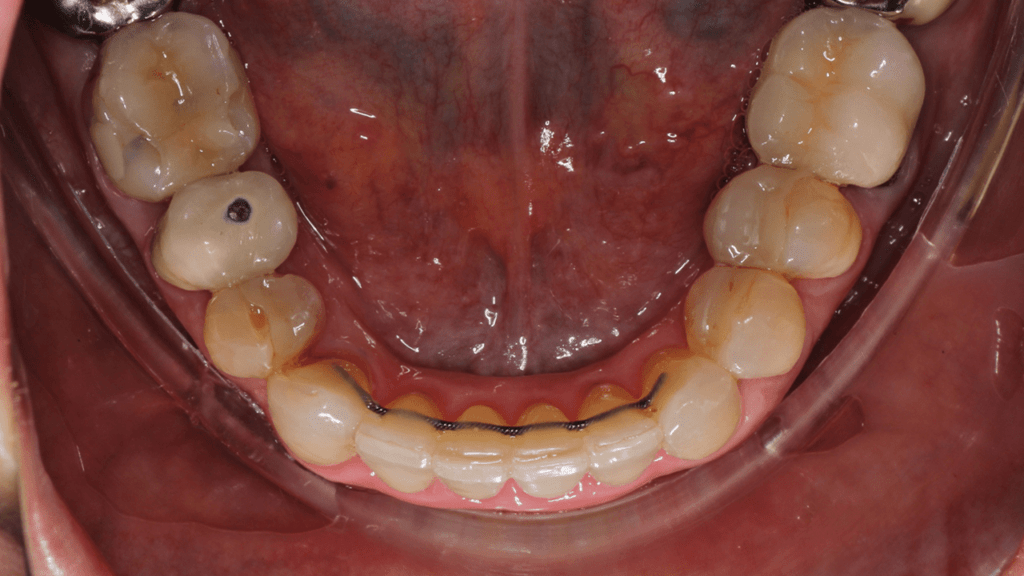
Challenges in Correcting Severe Rotations
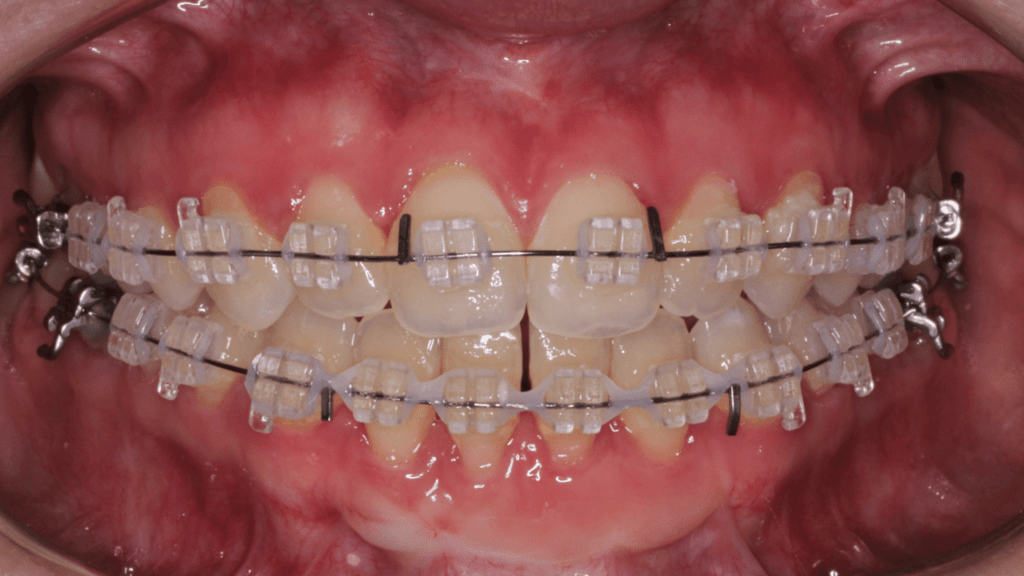
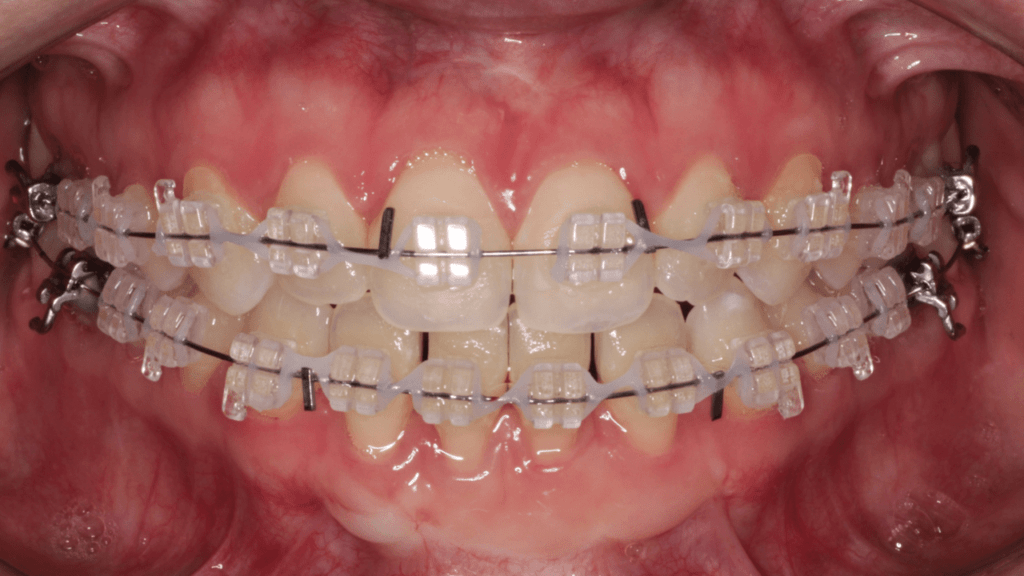
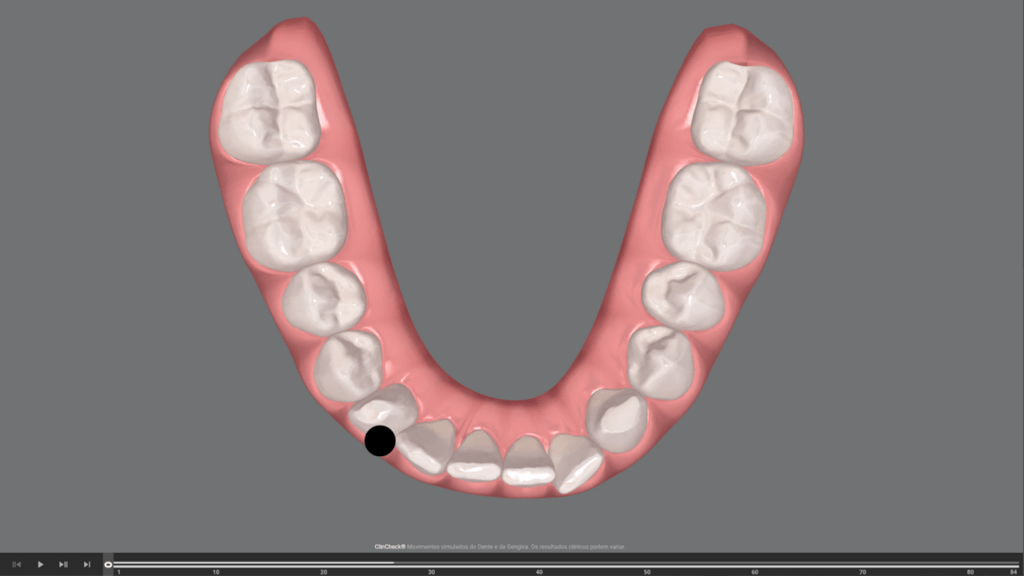
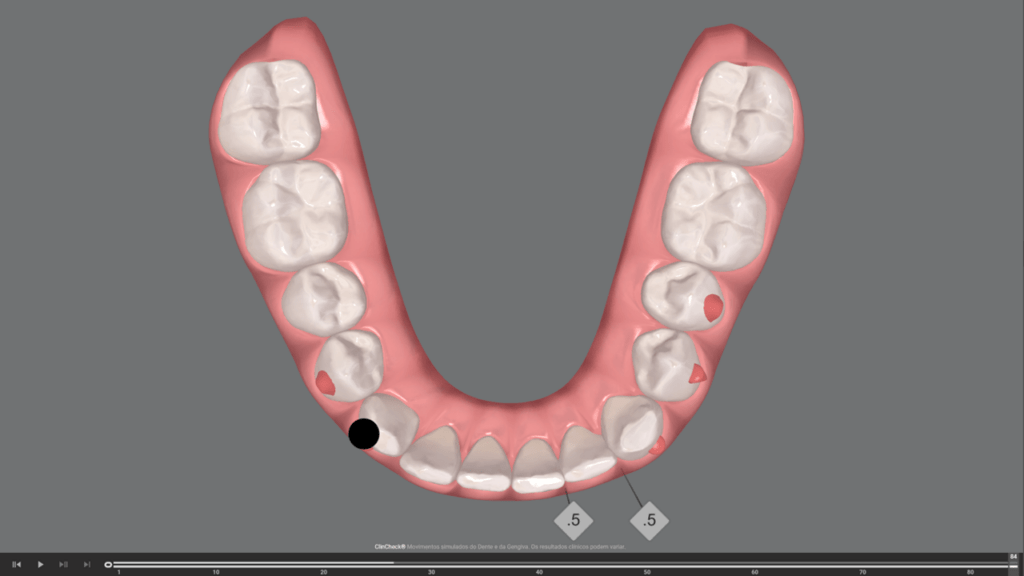
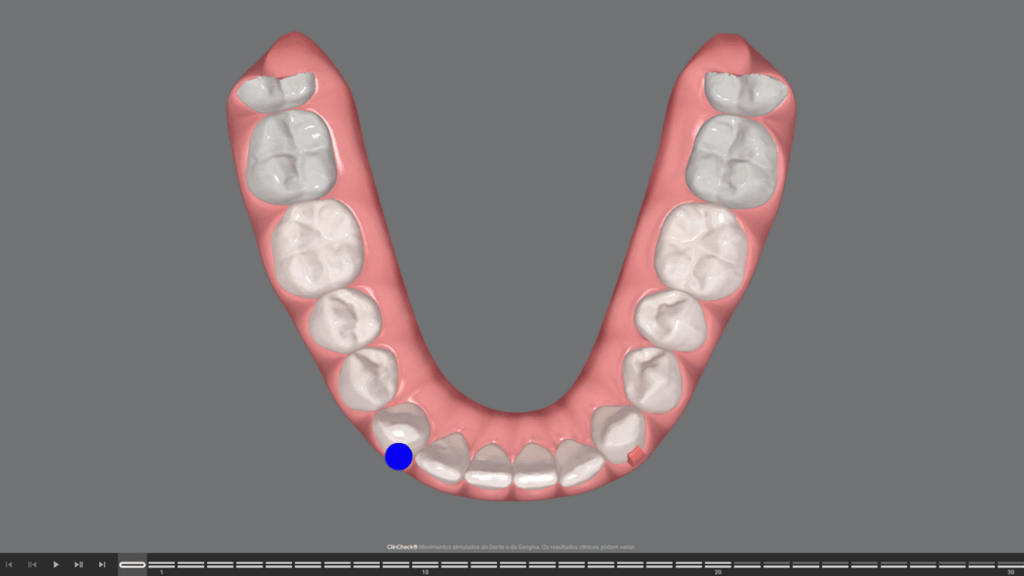
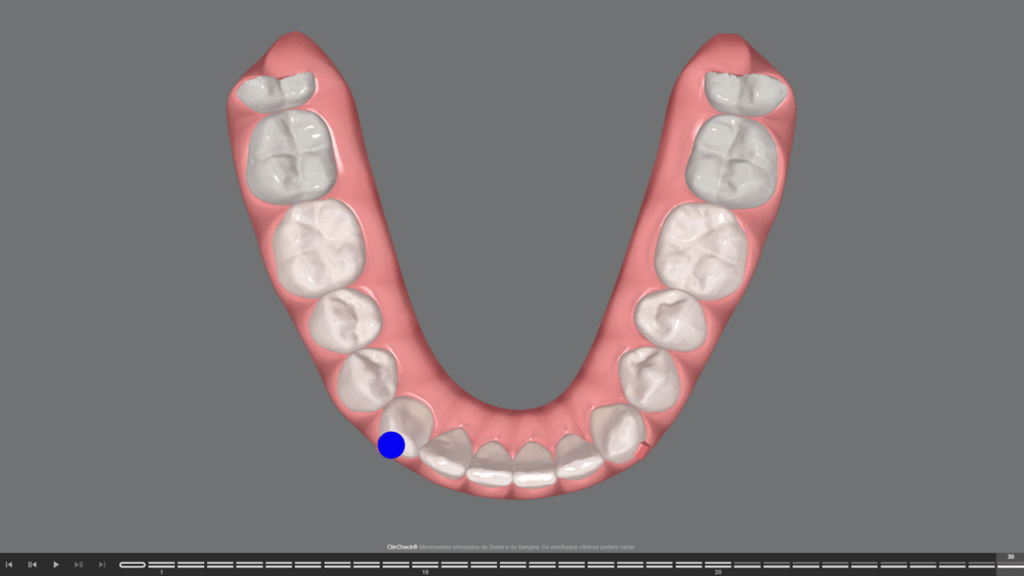
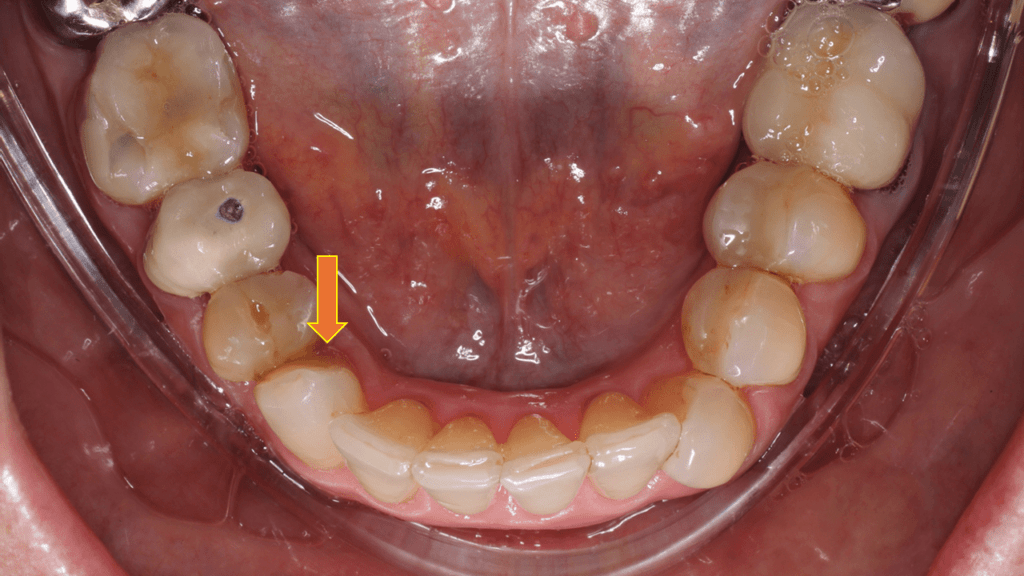
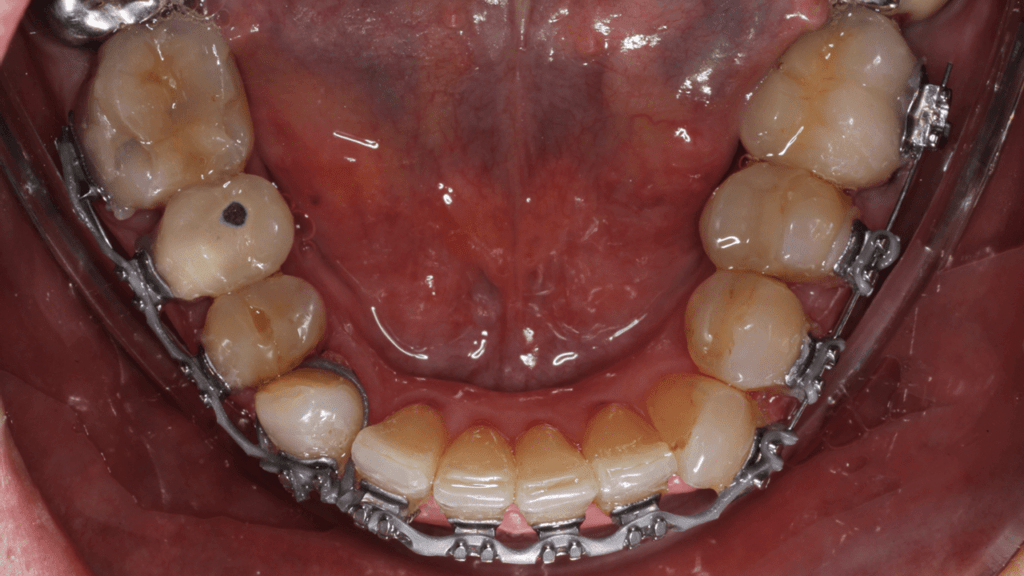
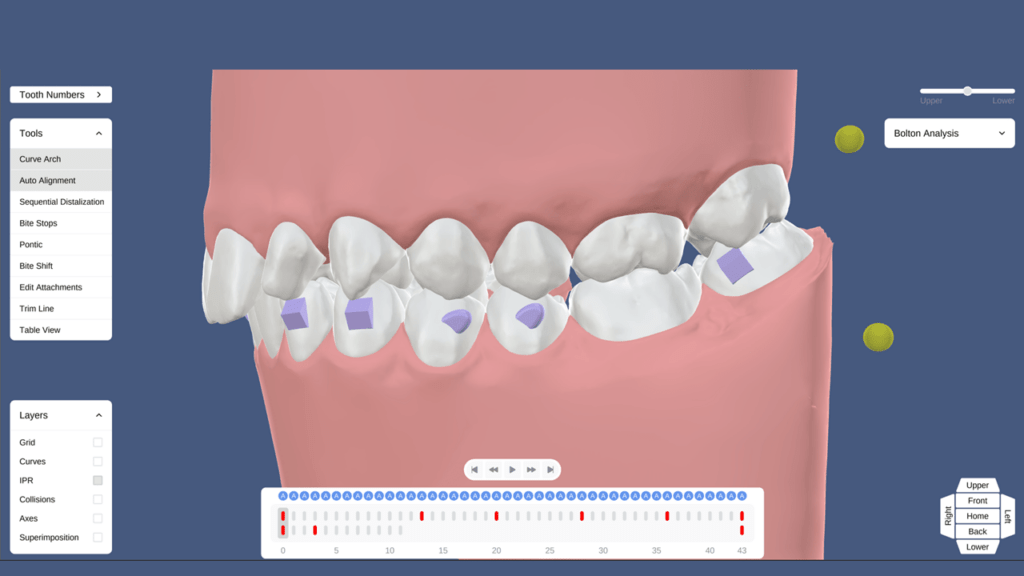
The correction of severe rotations is particularly challenging to manage with aligners,2,5,6,9 especially in premolars and canines.2,9,10 To improve the reliability of corrections, strategies such as intentional overcorrection,5,16-18 decreasing the velocity of movement5 and/or refinements13,19 should be utilized. While it is technically possible to achieve significant rotational corrections with aligners, the time required is a critical factor. Without sufficient time, patient compliance might compromise the final outcome of the treatment. Although achieving rotations exceeding 60 degrees with aligners alone is feasible, (FIGURE 2 and 3) the prolonged treatment duration required may not be practical or reasonable.
Figure 2 – Patient Outcomes for Severe Rotation Correction

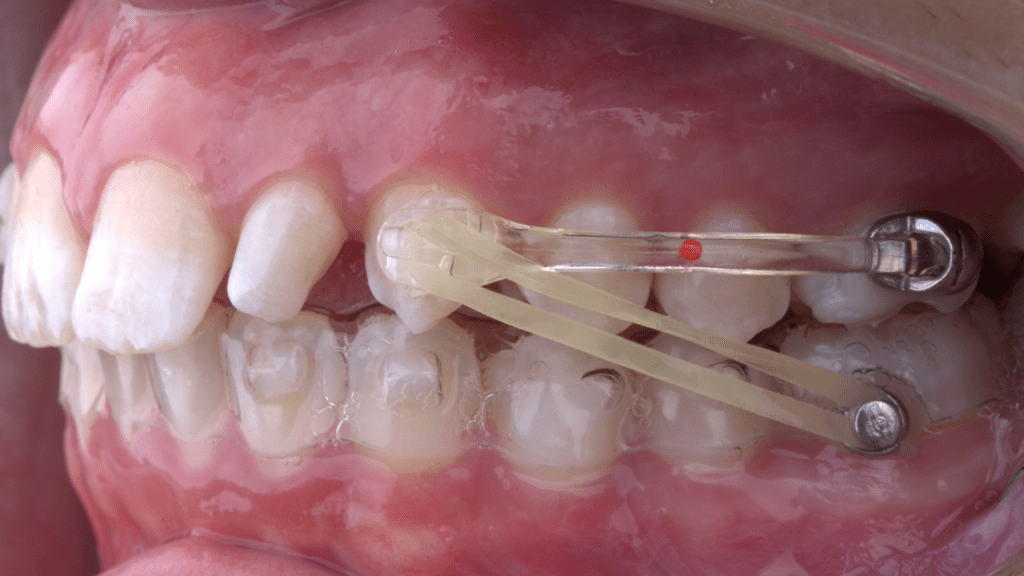
Figure 3 – Planning and Treatment Progress for Figure 2 Patient
In contrast, fixed appliances typically can correct rotations much more quickly compared to aligners. Fixed appliances’ biomechanical benefits are notable, as they can apply consistent and continuous forces around the clock, allowing for more efficient and effective rotation corrections. While we are not considering the aesthetic advantages of aligners in this context, these properties make brackets highly effective for treating severe rotations.
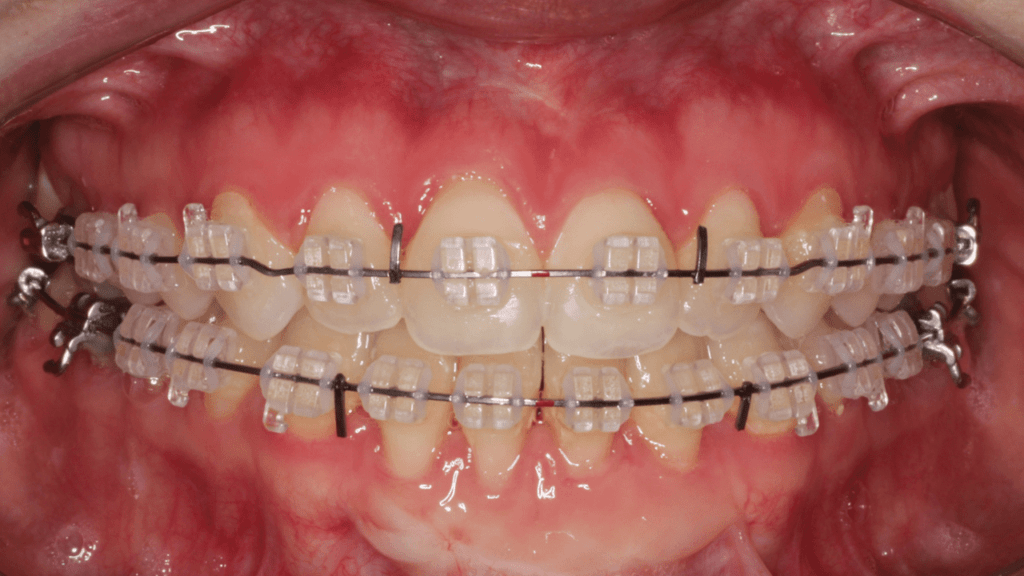
Therefore, in situations where severe rotations are present, it might be advantageous to initially correct these using fixed appliances over a span of 3-4 months. After addressing the severe rotations, transitioning to aligners can be beneficial for completing the remainder of the treatment, leveraging their aesthetic appeal and patient comfort. (Figure 4)
Figure 4 – Hybrid Treatment Overview
Effectiveness of Aligners in Distalization
Aligners can be effective in achieving anterior-posterior (AP) correction.2,5 Although the reliability of this correction varies widely, with accuracy reported between 7% and 88% according to the literature2,20,21 aligners can predictably distalize maxillary molars by up to 1.5 mm.2,5 In addition to the sequential distalization of the maxillary dentition, simultaneously promoting the mesialization of the mandibular dentition can enhance treatment outcomes. To achieve this effectively, additional mechanics should be employed, such as intermaxillary elastics or intramaxillary elastics with skeletal anchorage. However, the key consideration is not only whether aligners will successfully achieve the desired AP correction, but also the duration required for these movements to occur. Understanding this timeline is crucial for orthodontists to plan treatment effectively and manage patient expectations.
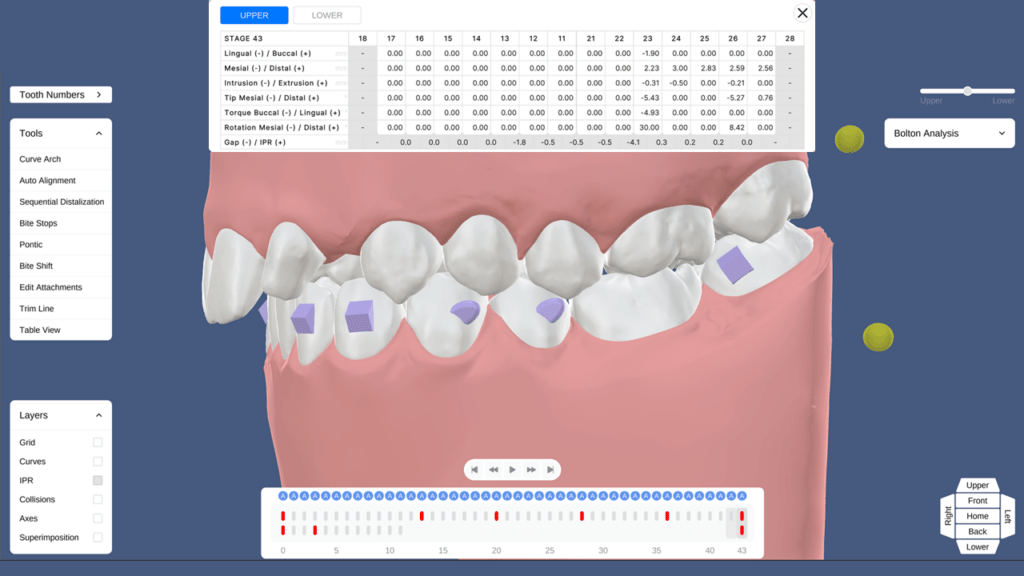
Mesio-distal movements programmed for each aligner are typically around 0.2 mm per aligner. The distalization protocol often employs a 50-50 movement strategy, where each tooth begins to move only after the preceding tooth has achieved 50% of its targeted movement. For example, the first molar will begin to distalize once the second molar has reached 50% of its intended distalization, and this pattern continues sequentially. This method often requires approximately 45 aligners to achieve a total distalization of 2 to 2.5 mm. Assuming patients change their aligners every 14 days, the distalization process for molars, premolars, and canines is expected to take approximately 22 months. (FIGURE 5)
Figure 5 – Estimation of Sequential Distalization of Maxillary Molars, Premolars, and Canines
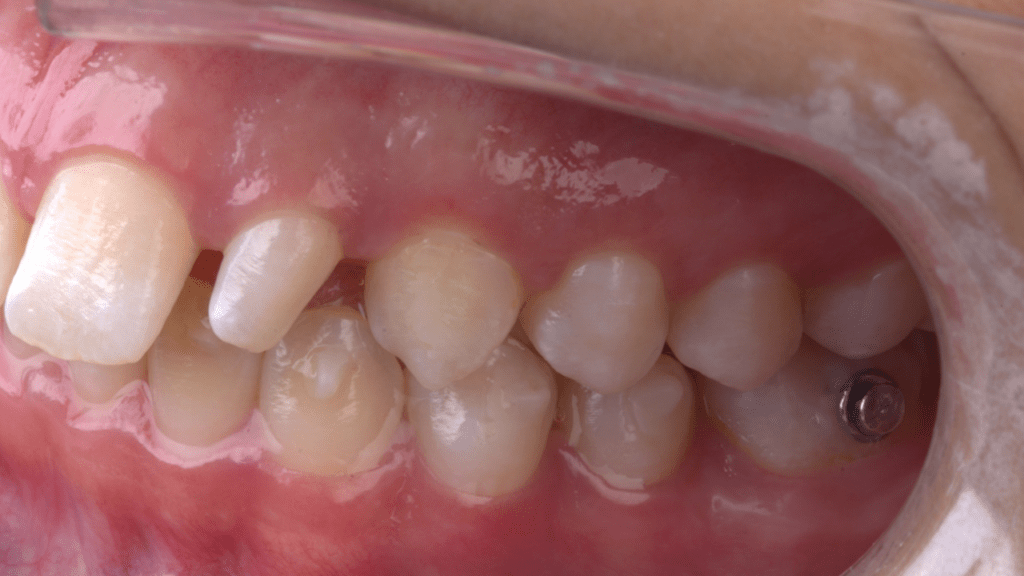
In contrast, alternative methods such as ‘Carriere’-style distalizers or traditional fixed appliance mechanics can achieve equivalent results much faster, typically within 3 to 6 months of treatment. These approaches offer significant advantages in terms of time efficiency, allowing for quicker corrections and potentially improving patient satisfaction with the overall treatment timeline. Once the planned anterior-posterior (AP) corrections are achieved, the patient can transition to aligner treatment, which will require fewer aligners. This strategy not only speeds up the treatment process but also reduces costs, making it a more efficient option for both practitioners and patients. (Figure 6)
Figure 6 – Distalization Using Hybrid Orthodontics in a Case with Undesired Proclination of Incisors
Conclusion
In summary, while aligners provide a more practical and aesthetic approach for patients compared to fixed appliances, they face significant limitations in controlling complex tooth movements such as severe rotations, extrusion of anterior teeth, and achieving timely distalization. Their reliance on patient compliance and the nature of the material often lead to challenges in achieving timely and predictable outcomes. In contrast, fixed appliances, with their ability to apply continuous forces and produce reliable load systems, allow for more efficient and effective corrections, particularly for challenging movements.
The hybrid treatment approach leverages the strengths of both fixed appliances and aligners. By initially utilizing fixed appliances to manage complex movements, orthodontists can establish a solid foundation for treatment. Once difficult movements are simplified and time-consuming issues are resolved, transitioning to aligners allows for the delivery of final adjustments while also enhancing the aesthetic appeal and comfort for patients.
Ultimately, the strategic integration of both treatment modalities not only improves overall treatment outcomes but also aligns with patient preferences for enhanced aesthetics and comfort. This comprehensive approach exemplifies the evolving landscape of orthodontics, where the synergy between traditional mechanics and innovative technology can fulfill the clinical needs and expectations of modern patients.
References
1. Taffarel IA, Gasparello GG, Mota-Junior SL, Pithon MM, Taffarel IP, Meira TM et al. Distalization of maxillary molars with Invisalign aligners in nonextraction patients with Class II malocclusion. Am J Orthod Dentofacial Orthop 2022;162:e176-e182.
2. Rossini G, Parrini S, Castroflorio T, Deregibus A, Debernardi CL. Efficacy of clear aligners in controlling orthodontic tooth movement: a systematic review. Angle Orthod 2015;85:881-889.
3. Jiang T, Jiang YN, Chu FT, Lu PJ, Tang GH. A cone-beam computed tomographic study evaluating the efficacy of incisor movement with clear aligners: Assessment of incisor pure tipping, controlled tipping, translation, and torque. Am J Orthod Dentofacial Orthop 2021;159:635-643.
4. Drake CT, McGorray SP, Dolce C, Nair M, Wheeler TT. Orthodontic tooth movement with clear aligners. ISRN Dent 2012;2012:657973.
5. Simon M, Keilig L, Schwarze J, Jung BA, Bourauel C. Treatment outcome and efficacy of an aligner technique–regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health 2014;14:68.
6. Upadhyay M, Arqub SA. Biomechanics of clear aligners: hidden truths & first principles. J W 2022;J World Fed Orthod:12-21.
7. Galan-Lopez L, Barcia-Gonzalez J, Plasencia E. A systematic review of the accuracy and efficiency of dental movements with Invisalign(R). Korean J Orthod 2019;49:140-149.
8. Kravitz ND, Kusnoto B, BeGole E, Obrez A, Agran B. How well does Invisalign work? A prospective clinical study evaluating the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop 2009;135:27-35.
9. Haouili N, Kravitz ND, Vaid NR, Ferguson DJ, Makki L. Has Invisalign improved? A prospective follow-up study on the efficacy of tooth movement with Invisalign. Am J Orthod Dentofacial Orthop 2020;158:420-425.
10. Kravitz ND, Kusnoto B, Agran B, Viana G. Influence of attachments and interproximal reduction on the accuracy of canine rotation with Invisalign. A prospective clinical study. Angle Orthod 2008;78:682-687.
11. Khosravi R, Cohanim B, Hujoel P, Daher S, Neal M, Liu W et al. Management of overbite with the Invisalign appliance. Am J Orthod Dentofacial Orthop 2017;151:691-699 e692.
12. Harris K, Ojima K, Dan C, Upadhyay M, Alshehri A, Kuo CL et al. Evaluation of open bite closure using clear aligners: a retrospective study. Prog Orthod 2020;21:23.
13. Robertson L, Kaur H, Fagundes NCF, Romanyk D, Major P, Flores Mir C. Effectiveness of clear aligner therapy for orthodontic treatment: A systematic review. Orthod Craniofac Res 2020;23:133-142.
14. Kim YH. Anterior openbite and its treatment with multiloop edgewise archwire. Angle Orthod 1987;57:290-321.
15. Kucukkeles N, Acar A, Demirkaya AA, Evrenol B, Enacar A. Cephalometric evaluation of open bite treatment with NiTi arch wires and anterior elastics. Am J Orthod Dentofacial Orthop 1999;116:555-562.
16. Palone M, Pignotti A, Morin E, Pancari C, Spedicato GA, Cremonini F et al. Analysis of overcorrection to be included for planning clear aligner therapy: a retrospective study. Angle Orthod 2023;93:11-18.
17. Al-Nadawi M, Kravitz ND, Hansa I, Makki L, Ferguson DJ, Vaid NR. Effect of clear aligner wear protocol on the efficacy of tooth movement. Angle Orthod 2021;91:157-163.
18. Charalampakis O, Iliadi A, Ueno H, Oliver DR, Kim KB. Accuracy of clear aligners: A retrospective study of patients who needed refinement. Am J Orthod Dentofacial Orthop 2018;154:47-54.
19. Lombardo L, Arreghini A, Ramina F, Huanca Ghislanzoni LT, Siciliani G. Predictability of orthodontic movement with orthodontic aligners: a retrospective study. Prog Orthod 2017;18:35.
20. Mamani J, Sessirisombat C, Hotokezaka H, Yoshida N, Sirisoontorn I. Effectiveness of Clear Aligners on Sequential Maxillary Molar Distalization: Discrepancy between Treatment Goal and Outcome. J Clin Med 2024;13.
21. Liu F, Liu J, Guo M, Li Z, Shu G, Dai F. Miniscrew anchorage versus Class II elastics for maxillary arch distalization using clear aligners. Angle Orthod 2024;94:3836-3391.