Non-surgical Orthodontic Treatment of a skeletal open bite Class II Division 1 malocclusion using The OnBRACE® System
Michael S. Johnston, DMD, MS, ABO-Board Certified
INTRODUCTION
Open bite treatment, especially non-surgical treatment of skeletal open bites, with fixed orthodontic appliances represents a significant challenge to the orthodontist. Orthodontic mechanics that cause molar extrusion need to be minimized throughout treatment. Fixed orthodontic appliances such as maxillary expanders are known to produce molar extrusion as well as downward and forward movement of the maxilla; thereby imparting a wedge-effect and worsening the anterior open bite. The OnBRACE® molar appliance prevents molar extrusion and additionally produces 1 mm of molar intrusion, thus promoting open bite correction.
DIAGNOSIS AND ETIOLOGY
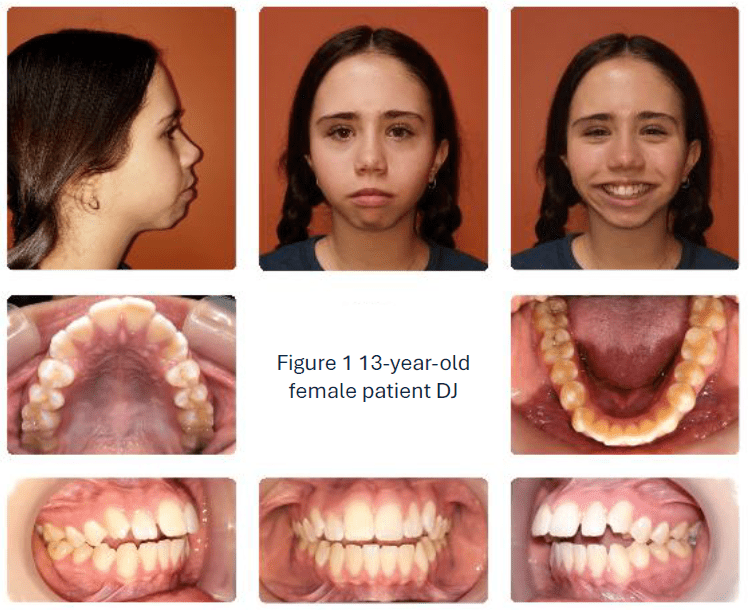
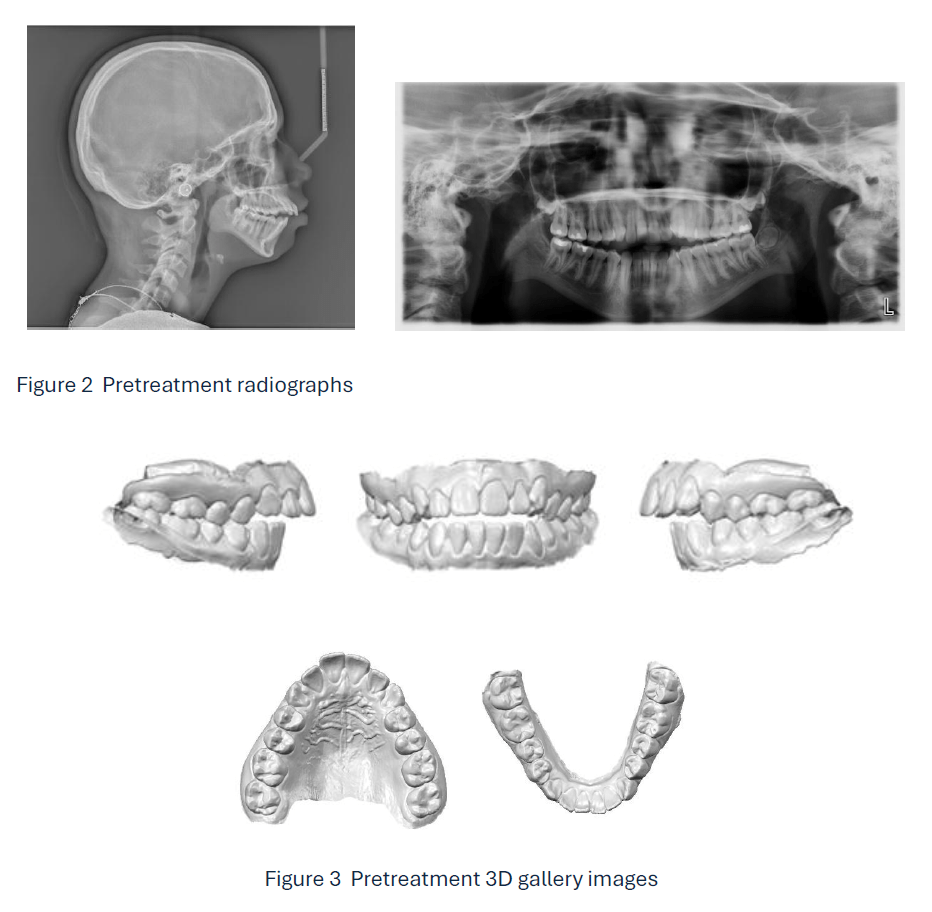
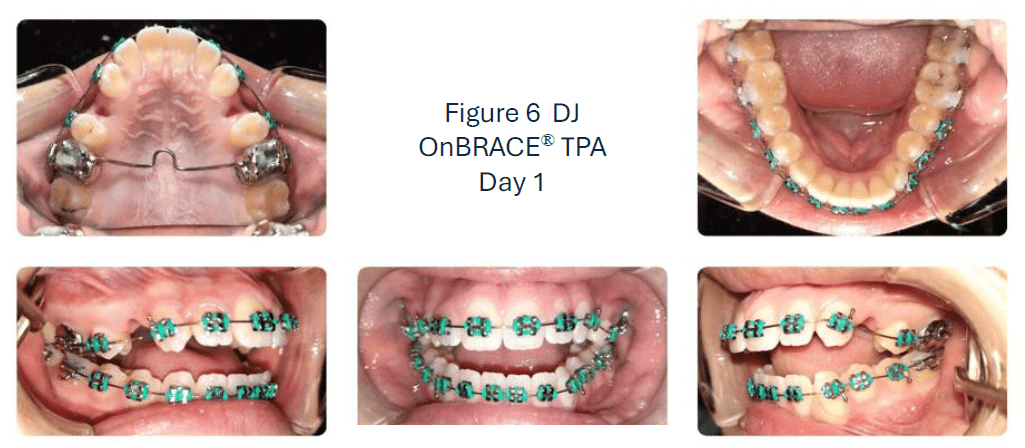
Patient DJ is a 13-year-old female who presents with a hyperdivergent mandibular plane angle, mandibular retrognathia, maxillary protrusion, Class II Division 1 malocclusion, 3 mm skeletal anterior open bite, 10 mm overjet, 1 mm CR/CO discrepancy, and lip incompetency with mentalis strain (Figs 1, 2, and 3). Thin attached gingiva on the facial of the mandibular incisors exists in an otherwise healthy periodontium. The patient does experience intermittent TMD symptoms with discomfort. The patient was 3 years post-menarcheal.
TREATMENT OBJECTIVES
Comprehensive orthodontic treatment objectives for this patient were to maintain the mandibular plane angle by controlling molar vertical dimension, achieve proper overbite and overjet, reduce maxillary incisor protrusion, improve lower incisor inclination, achieve a stable and functional occlusion, and improve lip competency.
TREATMENT ALTERNATIVES
Class II fixed functional appliances like the MARA and Herbst appliances were ruled out due to the patient being 3 years post-menarcheal, having a hyperdivergent mandibular plane angle and exhibiting thin attached gingiva on the lower incisors.
Postponing orthodontic treatment to allow for future orthognathic surgery was discussed with the parents and patient. A future orthodontic/orthognathic surgical option was declined by the parents.
A non-surgical, extraction, orthodontic treatment was planned for DJ which included full fixed orthodontic appliance therapy, OnBRACE® TPA for vertical control and maximum anchorage, extraction of the upper first premolars and lower interproximal reduction.
TREATMENT PROGRESS
Full fixed orthodontic appliances, 0.022” X 0.028” metal Roth Rx mini twin bracket, were placed and the digital scan of the patient was sent to the lab for OnBRACE® TPA fabrication. Extraction of the unbonded upper first premolars was completed.
The OnBRACE® (Fig. 4) is a unique metal laser-sintered fixed orthodontic appliance that saddles the posterior tooth without interproximal metal intrusion thus eliminating the need for orthodontic separators. Occlusal coverage with the OnBRACE® provides molar intrusion that is advantageous for open bite cases as well as providing a bite turbo effect for deep bite cases.

Figure 4

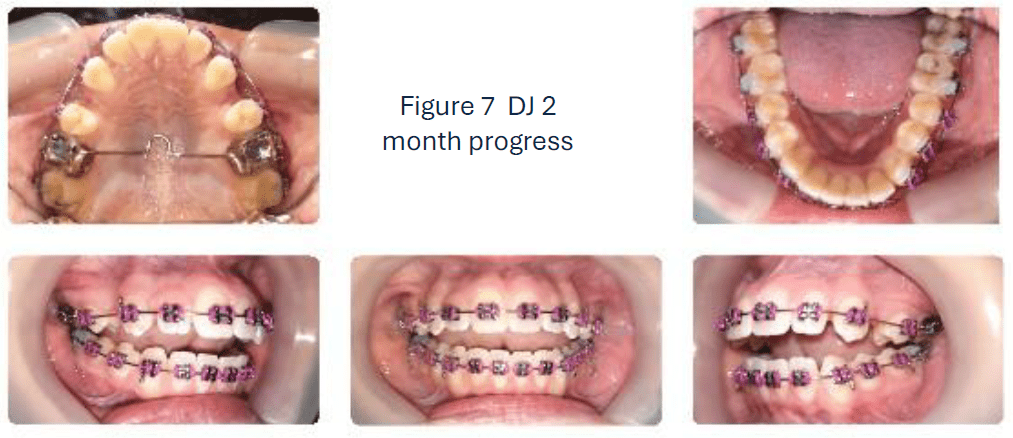
Figure 5 OnBRACE® TPA Day 1
An OnBRACE® TPA (Fig. 5) was cemented to the upper first molars to provide maximum anchorage to prevent molar extrusion and maintain molar A-P position.
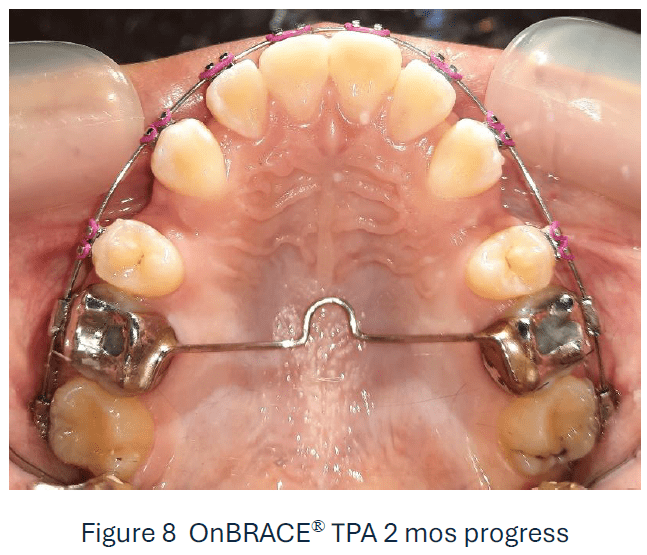
Initial placement of the OnBRACE® TPA does transiently increase the anterior open bite (Fig. 6). As the metal occlusal coverage of the OnBRACE® provides intrusion of the first molars, resultant overbite correction will be achieved partially by mandibular autorotation following appliance removal. The maxillary second molars should be bonded at placement of the appliance, or an occlusal rest should extend to the second molars in order to prevent super-eruption of the second molars.
Initial leveling and aligning was completed using 0.016”, 0.018”, 0.020” Heat-activated NiTi archwires sequentially. Space closure was completed on 0.019” X 0.025” Heat-activated NiTi archwires. An upper 0.019” X 0.025” stainless steel wire was secured at month #7 while lower 0.019” X 0.025” HA NiTi archwire was maintained on the lower arch.
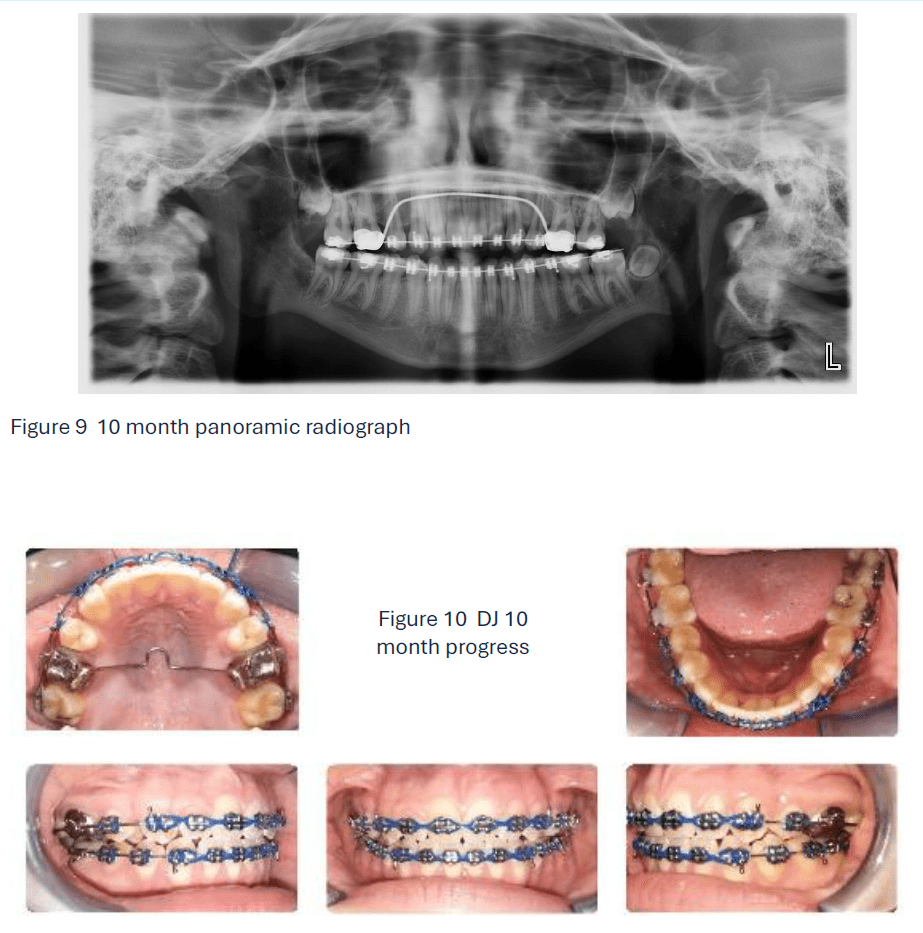
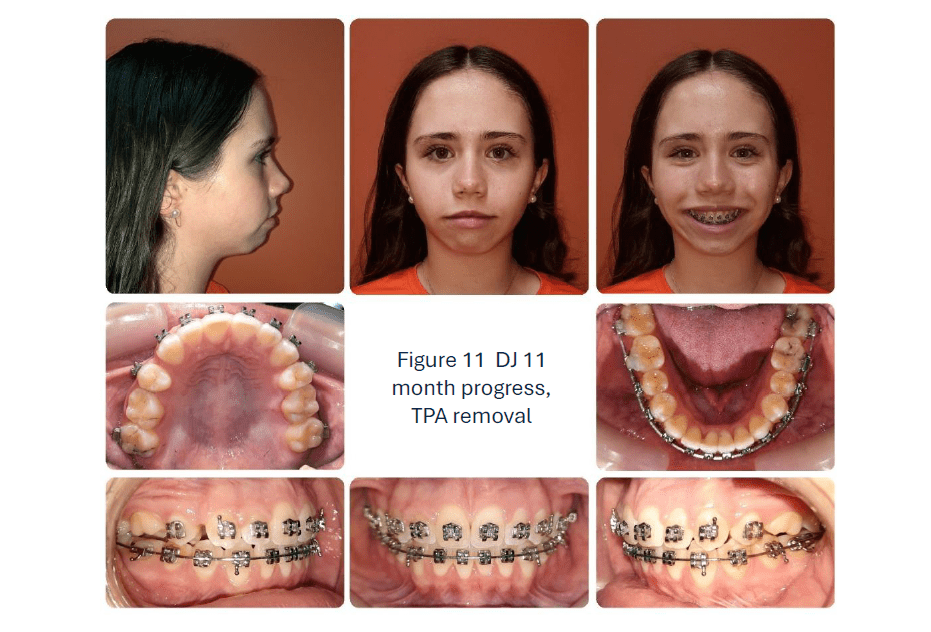
An upper 0.021” X 0.025” stainless steel archwire was placed at 8 months for full torque expression. Open bite closure has made significant progress with the OnBRACE TPA in place as seen in the 10 month records (Figs 9 and 10). Patient and parents are very pleased with the results to date.
At the 11 month appointment, the OnBRACE TPA was removed (Fig. 11) and the upper 6s were bonded.
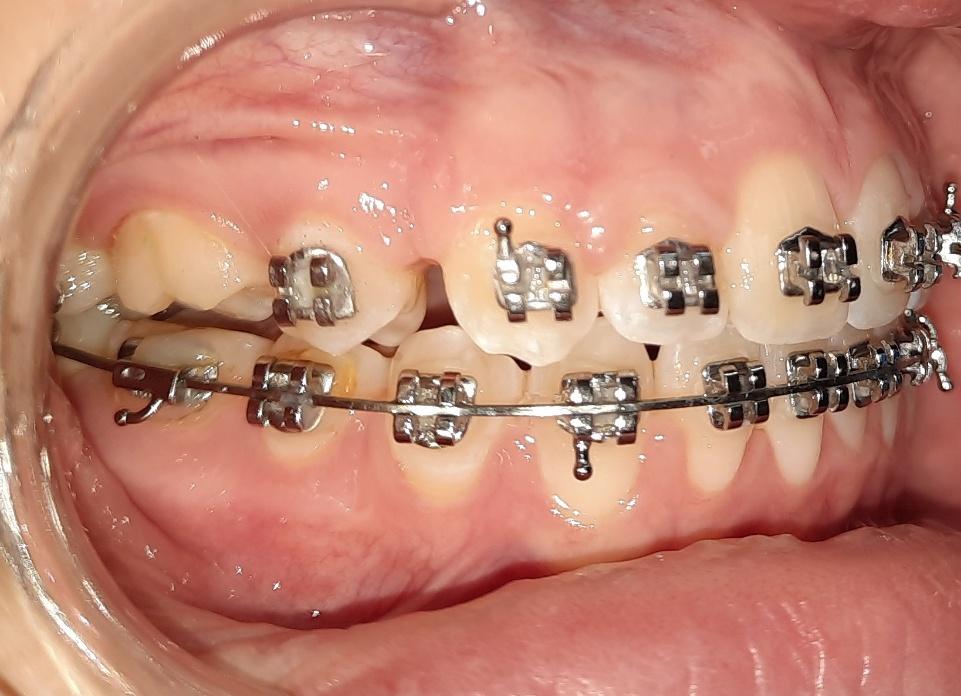
Figure 12 Maxillary right first molar intrusion evident clinically following appliance removal.
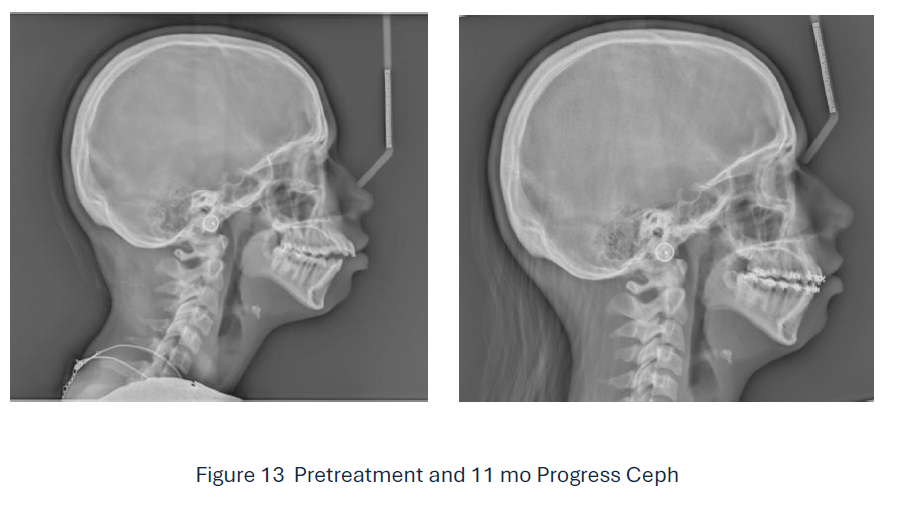
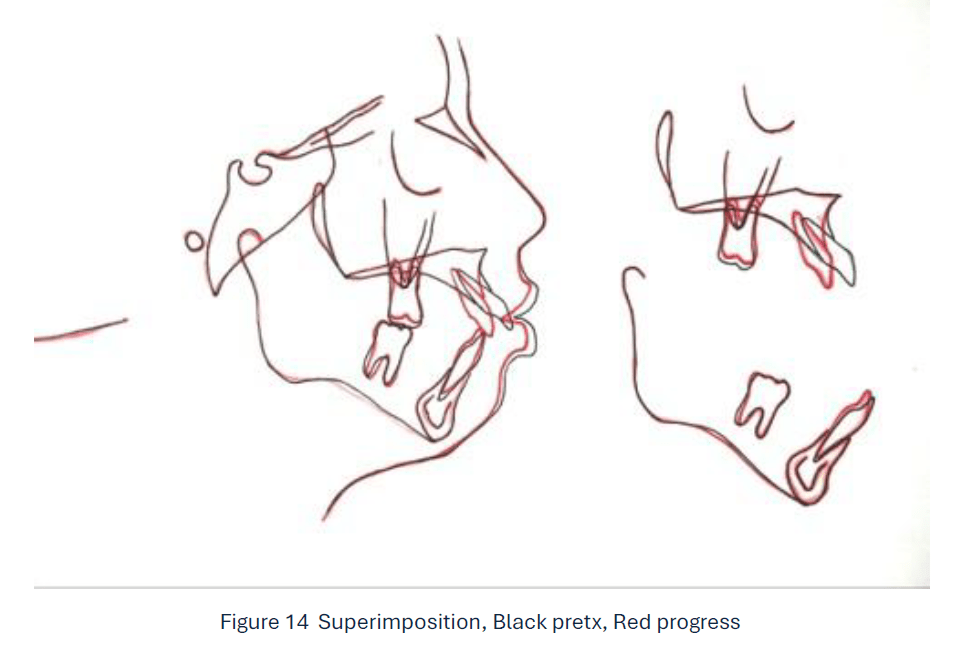
Superimposition of pretreatment and progress cephalometric radiographs (Figs 13 and 14) reveals approximately 1 mm of maxillary molar intrusion was achieved utilizing the OnBRACE® TPA for 11 months. Maximum A-P anchorage of the upper first molars was achieved with the OnBRACE® TPA. Lower molar extrusion was prevented, and the mandibular plane angle remained unchanged. Significant retraction of the upper incisors was achieved with minimal extrusion. Minor lower incisor retraction and extrusion was seen. Treatment is currently ongoing with detailing and finishing.
CONCLUSION
The OnBRACE® fixed appliance is an innovative orthodontic appliance that provides effective maxillary molar intrusion. Case DJ exhibits maximum anchorage and molar intrusion achieved with the OnBRACE® TPA. The OnBRACE® provides many advantages with other appliances as well, including maxillary expansion appliances.
AUTHOR
Dr. Michal S. Johnston, DMD, MS, ABO-Board Certified is in private orthodontic practice in Greer, SC and is the inventor of the OnBRACE®. He has used the OnBRACE® on over 165 patients with appliances ranging from Hyrax expanders, MARA appliances, Herbst appliances, TPAs, LLHAs, Habit appliances, MARPE appliances, and individually.
DISCLAIMER
The author does have a financial interest in the OnBRACE® which is available at Specialty Appliances.